
The big low back curvature page… Brett’s Syndrome
Disclaimer: You are here probably because your new chiropractor Dr. Carr said you have this “Syndrome” and now you are (hesitantly) reading this. First off, I like to call it “Brett’s Syndrome”, after the man who introduced him to the concept; if you Google this condition you’ll find nothing, except maybe this page!
We just found an old video we made about this subject, if you’re feeling lazy.. just watch this!
or this!
So, where to begin? There are a number of entry points: Maybe you are the classic low back pain that comes through the door, or maybe you have a clear disc injury, or maybe Dr. Carr just diagnosed you with some weird tests, like seeing if you:
- can flatten your low back against a flat surface,
- checking your hamstrings,
- making you do the “sphinx” position from yoga, and
- checking your belly button to see if you have a hernia there… Crazy, huh? 🙂
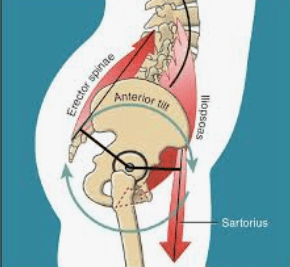
TL;DR :, it’s that you use an internal muscle group called the iliopsoas muscle to hold your low back together.
The “psoas” part of this muscle group, often called the “hip flexor”, attaches to the front of each lumbar vertebra bones and the discs of the lumbar/ low back spine. It’s partner muscle, the “iliacus” muscle, attaches inside your pelvic brim and runs down to the front of the femur. The reason we call them the iliopsoas is that the tendon is shared, like your Achilles tendon in your calf.
How’d you get this issue? Got any theories?
When we were toddlers, going from crawling to walking, we had to decide how we were going to hold our low back together. It turns out that instead of using the “outer” muscles of your core, you chose involuntarily to use the iliopsoas group to gain stability. While it’s possible to use these muscles to stabilize our spine, it’s not IDEAL. They are very compressive, pulling straight down the spine, crushing the discs between the back bones, often causing disc injuries. The muscle often pulls so long, so hard, that it often pulls a part of the bone literally off, where it can be seen on x-ray(!!). it can even close down the opening between the vertebrae, choking the nerve from a condition we call stenosis. For an initial primer on stenosis, you can look at our stenosis primer for patients page.
Below there are some pictures of what we see, and what we see that causes the issues we’re talking about.
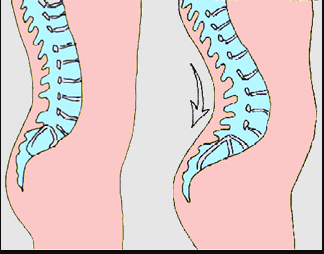

When the compression of the spine happens, it really only allows the spine to move forward, resulting in a rounding out of the low back, (picture #1) and an inability to flatten the spine (hence the “door test”). (Picture #2) It can often curve a patient’s belly out so much that, (if they aren’t working on their abdominal muscles through their lifetime) it will stretch along the line of tissue between their “6-pack muscles”, which shows up on situps like a vertical football shape we call diastasis recti. A continuation of this same hernia can be reflected in the belly button, resulting in a hernia there. Diastasis recti is totally normal in 3rd trimester pregnancies… any other time, it’s not.
The strange part of this condition is that many people who have this condition are often into precocious athletes younger in life. This is probably due to their spine being “pre-bent” into extension, or the “athletic position”: curved low back, glutes and quads and hamstrings firing, pelvis tilted forward.
However, this constant curve forward also means that the hamstring group in the back of the leg is forced to work as stabilizer muscle, working opposite to the iliopsoas group. This constant neurologic firing also means that the hamstrings are constantly short, and when asked to perform a maximal effort, like sprinting in track, they are simply overloaded and often tear.
So here’s the classic patient:
- a curved low back as evidenced by the sphinx position in yoga
- an inability to flatten the low back against a flat surface
- short hamstrings
- diastasis recti
- umbilical hernia
- anterior osteophytes on lateral lumbar view
If you’re still reading this, there is really only one way to manage this whole syndrome:
THE ILIOPSOAS MUST BE STRETCHED, IN ALL 3 DIMENSIONS… CLICK HERE FOR THE VIDEO
These muscles need to be stretched GENTLY and FREQUENTLY UNTIL A BETTER WAY TO STABILIZE THE LOW BACK IS PRESENTED.
This is a pretty big underlying premise to our care and why it’s in ALL CAPS. Before we talk about how long it takes to stretch the iliopsoas, let’s talk about where REAL stability in the lumbar spine comes from, and it’s not what you think.
The low back SHOULD be stabilized by:
- the diaphragm,
- the oblique muscles of the abdomen, and
- the Kegel group/ pelvic floor muscles at the bottom of the pelvic floor.
Notice I didn’t include the six pack muscles or the back muscles? Crazy, right? Seriously though, we’d love to tell you all the details about this, but for now I’m merely asking you to trust me on this.
So… what’s the treatment protocol for this?:
- ADJUST the low back into flexion. This gives the hinges in the low back the ability to move how we want them to.
- STRETCH the iliopsoas, in all three dimensions.
- TEACH PROPER BREATHING, using the diaphragm.
- WORK THE KEGELS.
- WORK THE OBLIQUES.
- MEASURE progress.
It’s been clinical experience that 16 times a day, for 16 weeks, is a good guideline for treatment length… after all, you have been doing this since you were a toddler.
16x a day, x 7 days per week x 16 weeks = 1792 stretch instances. The stretch takes about 30 seconds, so… 896 minutes. Divided by 60 minutes per hour, and it’s pretty doggone close to 15 hours of total time spent stretching.
You can do this!!
After all, let’s talk about all the UPSIDE to this care beyond getting rid of pain.
- Your back pain will go away
- You’ll be taller
- You’ll be faster
- You’ll be stronger in sports
- You’ll be better in bed
- You’ll be better looking naked
- You’ll be more oxygenated
- You’ll have more energy
- You’ll have stronger (and more control over) your orgasms (!)
- You’ll have a flatter stomach
- Your hamstrings will magically elongate
Is this not enough? With all the upside, and especially compared to the downside, this really is a no-brainer, and with the objectivity of the tests we do to see your progress, you can see the changes occur. This point of entry page is just the beginning, and it’s the place where you can have some of the questions answered about your syndrome before talking to Dr. Carr again.
Thanks for your time… you are on the right path here!