
Lumbar disc and reading the MRI
The Lumbar Disc and MRI’s
Please email the doctor if you have further questions… this article is in way a substitute for an evaluation and diagnosis by an actual doctor. The internet is not a doctor.
The opinions expressed here are strictly those of Dr. Peter Carr, downtown Seattle chiropractor.
So you found this page after being directed here from an internet search, or by an MRI that you wanted help reading. The purpose of this page is to give rational explanations of what the disc is, how it works, how it becomes damaged, what reports from radiologists say, and what that actually means to the patient the images were taken of. Finally, I’d like to talk about conservative treatment of the disc, and traditional allopathic (M.D.) solutions.
The structure of the lumbar disc
The lumbar disc is actually a ligament that holds the low back bones, called vertebrae, together. Because it also acts as a pad, separating the bones, it is exposed to some pretty disparate forces… it’s a lot like asking a coil of rope to work as a cushion, then alternating the cushion to work as a rope.
The lumbar disc has to support the weight of the enitre body and all of the structures above it, yet still allow for lots of motions in all directions that we make with our necks.
The lumabr disc, when looked at from the top, looks somewhat kidney bean-shaped. In the middle of the “bean” is a goopier substance called the nucleus pulposis, which in Latin means “pulpy center”.
The nucleus helps disperse loads from above, and it does that by being held in place by layers, or rings, of ligament, called the annular rings. Each layer/ ring has a diagonal arrangement that is opposite to the one above and below it, forming this really cool cross-matrixing net that normally holds the nucleus in the center.
Trauma, both microtrauma (posture/ running/ heavy vibration/ roller coasters/ pillows etc) and macrotrauma (car accidents/ football hits/ boxing/ falls) can tear the fibers of disc, allowing the more goopy nucleus to bow out that area. These bulges can go in any direction: forward, backward, sides, or any combination of those.
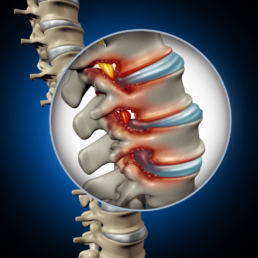
It’s only when the disc bulges backward that the real problems start to occur, and this is due to the anatomy involved: Right behind the disc is a vertical thin ligament called the posterior longitudinal ligament, that lines the tube formed by the vertebrae, where the spinal cord runs vertically.
The spinal cord is surrounded by fluid, called cerebrospinal fluid, that nourishes and protects the spinal cord, and the branches from it, called the spinal nerve roots, which exit the spinal column and transmit and receive all the strength and energy to and from our bodies. A look at the picture above showst a person from the perspective of someone standing to the right front of the spine we see.
A good analogy is to think of the lumbar spinal nerve roots is like a bunch of thin noodles, or a horse’s tail, surrounded by a sac. Better, think of a bunch of think noodles just outside a bag of water.
If your disc pushes hard enough, it will deform the bag (THECAL SAC), which COULD affect the nervous system. If it pushes on the noodles (spinal nerve roots), it WILL affect the nervous system at that level, and what that nerve influences in your body.
So to refresh:The spinal cord drops out of your head and goes through the tunnel formed by the bones of your spine.
Between each bone another hole is formed, called the IVF (intervertebral foramen) and a spinal nerve root peels away from the bunch of nerves and goes through that hole. The back part of the hole is called the lateral recess. If the disc closes down the IVF, that is termed stenosis.
Like all ligaments, the discs have no real blood supply after our teen years, and therefore have very little ability heal themselves. They do suck up water while we sleep, and slowly crush it away during the day, a hydraulic event called imbibition.
This is why we are shorter at the end of the day, and typically why people with disc injuries feel them more in the morning.
This seems like a good time to talk about symptoms, things that you feel or notice… when there is direct pressure on a nerve, either because of bone, disc, fat, or tumor, the nerve responds in one of two ways: it outputs too much information (pain, shooting pain, a deep gripping feeling) or too little (pins & needles / numbness / weakness / paralysis).
These areas of innervation are called dermatomes. Doctors use the weakness and /or loss of motor function as the dividing line between treatment and referral for surgery. Weakness, paralysis, or atrophy (the loss of muscle) are not good signs for recovery, and usually that’s when we send patients for MRI.
MRI is truly a miracle of our age. The giant magnets in an MRI force our hydrogen atoms to all spin the same plane, and when they turn off, the hydrogen emits some energy that the MRI unit reads and assigns a value to. Enough of them, and we can get a picture of what’s inside us. Unlike xrays, which really only look at “hard” things, MRI sees it all. Since you’re reading this, we’ll assume you have already had an MRI, and want to know what in the heck it means.
The rest of this information should be helpful when reading MRI reports. Always take the time to go through each word in the report.
And remember, there is no “good” or “bad”…it is what it is.
PHYSICAL STRUCTURES:
– Annular fibers/ annulus– Rings of ligaments that help to hold the nucleus pulposis in the center of the disc.
– Interspace– The height between vertebrae, an indication of relative disc health.
– Disc– A ligament that connects vertebrae together and keep them from coming apart.
– Lateral canal– the back end of the hallway through which the nerve exits the spine.
– Endplate– the top and bottom margins of the vertebral body, like the top and bottom of a can-shaped structure.
– Facet– The hinges of the spine, one on each side.
– Nucleus Pulposis– a “superball”-consistency center of a spinal disc which helps to disperse force.
– Osteophyte– Deposition of bone around another structure.
– Spurs/spurring– a sharp point of bones coming from a spinal structure
– Foramen/ foraminal– Any hole in a bone. When relating to the spine, it the IVF, or intervertebral foramen, a hallway formed by the vertebra above and below. This is where the spinal nerve root exits the spine.
– Spondyl- means “vertebra-related”.
– Marrow signal– The return on MRI of the tissue that makes blood inside the vertebrae.
– Osteophytes, as discussed above, are enlargements of that bone. It usually is referred to as arthritis of the disc, but that’s not accurate. It means that the bone is growing to stabilize your neck.
– Thecal sac– the membrane filled with cerebrospinal fluid that contains the spinal cord.
IMAGES:
T1/ T2– Ways to look at the information for MRI studies. In general, the MRI spins up all the hydrogen ions in the body, aligning their spins to one single plane. When released, the hydrogen returns to its old plane, releasing measurable energy.
T2 images show large amounts of hydrogen in white, showing tissues such as fat, and water.
DIRECTIONS/ RELATIONS:
– Anterior– towards the front
– Posterior– towards the back
– Superior– towards the head
– Inferior– towards the feet
– Distal– away from the centerline
– Proximal– toward the centerline
– Central– Goes directly posterior
– Paracentral– usually right or left… of center
– Retrolisthesis– a backward slippage
– Anterolisthesis– a forward slippage
– Extension – arching backward, bending backwards, up to the ceiling
– Flexion– bending forward toward the floor
– Lateral Flexion– sideways bending
– Lordosis– a forward facing banana curve of the vertebra, normal in the neck and low back
– Dermatome– an area of skin innervated mostly by one nerve. Help to diagnose levels of injury.
– Hypertrophy– an enlargement or thickening of
– Stenosis– closing down of a hole or holes (foramen)
– Bilateral– both sided
– Radicular/-radiculo– follows a classic pattern of nerves
CONDITION SEVERITY:
– Tiny– really, pretty small
– Mild – small
– Moderate– medium
– Severe– Large
– Marked– WOW!
– lysis – a breakage
– osis – a long-term inflammation of
– listhesis – a slippage
– pathy – there’s something wrong with whatever prefix came first
TYPES OF DISC INJURIES
– Protrusion– a direct bulging of the disc
– Bulge– a diffuse bulging of the disc
– Herniation– a frank and focal outpouring of the nucleus pulposis
– Extrusion– A pronounced protrusion
– Sequestered– a piece of the disc is floating free in the cerebrospinal fluid.
INDICATIONS THAT THINGS ARE HAPPENING:
– Encroachment– something is closing in on something else
– Ligamentous laxity– indicates a sprain, where the bones move too much on one another.
– Effusion– swelling, usually in response to inflammation
– Disc height– the distance between two vertebra, a good indication of disc health
– Disc desiccation– the amount of water contained in the disc structure
– Anterior osteophytes– a bony sign of degenerative disc disease, or a decay of the discs in your neck.
– When reading reports, there are the FINDINGS and IMPRESSIONS. USUALLY: the impressions section is numbered or “ranked” in order of severity.